
Dr Musa Mohd Nordin, Paediatrician
Dr Yap Wei Aun, Public Health Physician
Asst Prof Dr Farhan Mohammad Rusli, Public Health Physician
The Seventh Malaysia Plan (1996-2000) promised a new district hospital in Lawas. Kam Agong was pregnant with her eighth child in 2002. She was only 44 years old and otherwise in good health. But she died from excessive bleeding after delivering her child. 20 years after her death and the hospital remains an unfulfilled promise. High-risk pregnant women still needs to undertake long arduous journeys to either Miri or Kota Kinabalu for specialist care and caesarean sections.
Reforms of the healthcare system are long overdue and urgent. There have been 14 past studies since 1985, with near unanimous consensus, but yet reforms were amiss. [1]
What are the challenges to our health system?
Our past leaders had bequeath us a health system which performed above its expectations and was respected globally. In the previous century, deaths of pregnant women, infants, and children was relatively low given Malaysia’s economic status compared with countries at a similar economic development to us.
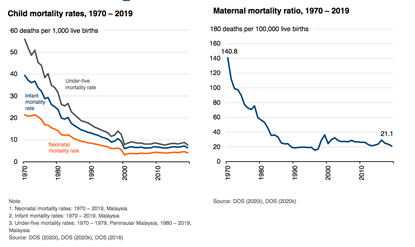
However, improvements in such critical indicators in the 21stcentury has stagnated—deaths among pregnant women, infants, and children made no discernable progress for the last two decades since 2000. (Diagram I)
Diagram I: Infant and Child Mortality Rates and Maternal Mortality Ratio from 1970-2019
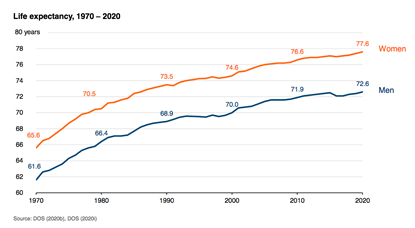
Similarly, although life expectancy has been improving, the pace of improvement in life expectancy among males who have reached the age of 60—a proxy for non communicable diseases—is glacial compared with comparator countries, leading to a yawning gap. There was only 11 years (male) and 12 years (female) gain of life expectancy over a 50-year period from 1970 to 2020. [5] (Diagrams II-IV)
Diagram II: Male Life Expectancy at Age 60 years: International Comparison

Diagram III: International Comparison of Life Expectancy 1990 and 2019
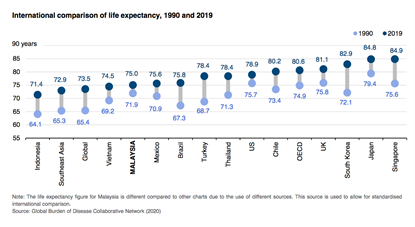
Diagram IV: Life Expectancy in Malaysia 1970-2020
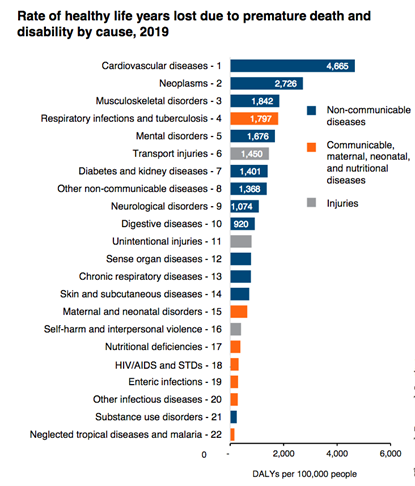
Furthermore, although Malaysians are living longer, they are not spending those extra years in good health. According to the 2019 National Health and Morbidity Survey, 1.7 million (8.1%) live with all the three NCDs and 3.4 million with two NCDs. 73.6% of total health loss was due to NCDs.[6][Diagram V-VII] [2,3]
Diagram V: Life Expectancy and Healthy Life Expectancy in Malaysia 1990-2019
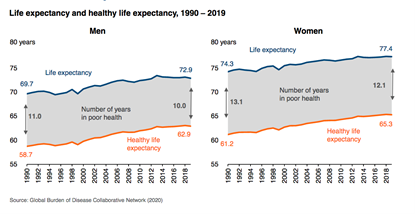
Diagram VI: Number of People in Malaysia living with 2 to 3 NCDs
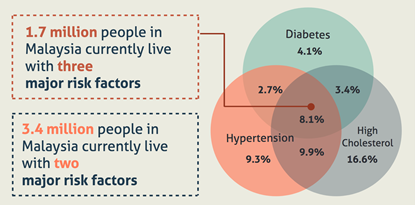
Diagram VII: Rate of Healthy Life Years lost due to Premature Death and Disability by Cause in 2019
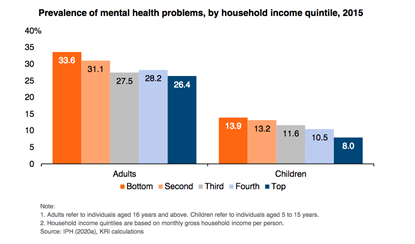
Inequalities in health are rife. The Khazanah Research Institute (KRI) reports wide inequalities. Life expectancy is shorter in states with lower incomes. Diabetes, hypertension and hypercholesterolemia are more prevalent in lower income groups. Mental health problems are more common in lower income families. Such data provide the evidence that the tragic stories such as Kam Agong are not mere anecdotes, but a systemic problem for Malaysia. (Diagram VIII-IX) [2]
Diagram VIII: Prevalence of diabetes, hypertension and hypercholesterolemia among adults by household income quintiles in 2015
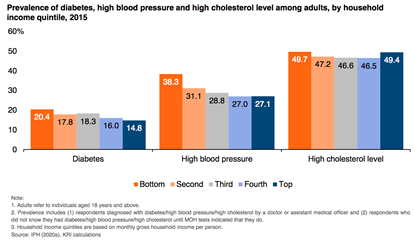
Diagram IX: Prevalence of mental health problems by household income quintiles in 2015
Much ink has been spilt to highlight the everyday experience of ordinary Malaysians faced with inadequate public investment in health—the Auditor General in 2018 reported that the hospitals were understaffed, overcrowded and underfunded [4].
Much praise has been heaped on our healthcare services—especially for hospitals which service expatriates and high income individuals—but the reality for the masses is that we are only ranked 84th on the Healthcare Access and Quality (HAQ) Index. The HAQ Index measures a person’s access to quality healthcare that would protect one from amendable mortalities due to 32 different diseases. [5]
And as diagram X illustrates, we are well behind our neighbors, Sri Lanka, Thailand, Singapore, Taiwan and Japan on the HAQ Index for the years 1990-2015.
Diagram X: Healthcare Access and Quality Index (HAQI), 1990-2015

Key determinants of the transformation of our nation’s health
As alluded to by researchers at the Khazanah Research Institute (KRI) as recently as April 2022, there is extensive evidence to show that societal factors such as education, housing, welfare, environment and occupation have a much greater impact on nurturing the public’s long term health. [6]
Often described as the social determinants of health; social, economical, commercial, environmental and educational conditions are undoubtedly the most powerful influencers of the people’s health. [7]
In as much as the reforms of the Ministry of Health is overdue, it is not the be all and end all of the state of the nation’s health.
We would be missing the forest from the trees if the nation is yet again led to think that a better and reformed MOH would transform the people’s health. The nation faces multiple challenges to reduce the health inequalities and improve the people’s health.
It is obvious from the KRI report that one of the most powerful drivers of good health is the ability to secure an adequate income. The COVID-19 pandemic has further amplified this problem. The number of families and children experiencing poverty has increased from a poverty rate at 5.6% in 2019, to at least to 8.4% of all households in 2020 due to the pandemic. [8]
We are very hopeful that the White Paper will reframe the national health agenda. The people’s health needs to be valued as an asset and health aspects must be considered by the government across all it’s policies. The government needs to drive policy decisions which would create social, economical, commercial, environmental and educational situations which creates healthy lives of it’s people.
Apart from the reformation of the healthcare system, these wider and more powerful social determinants of health must be prioritized and the inequalities in health addressed appropriately and urgently.
The social discriminants of health can only be successful if it is incorporated within the context of health in all policies (HiAP) of a whole of government approach. [9]
The HiAP government philosophy considers seriously the health implications of all public policies across all sectors and ensures that they synergize to enhance population and health equity and avoids harmful impacts on health.
One of the most difficult conundrums for a health reform agenda is the lack of or failure of multi-sectoral integration of agencies and relevant authorities.
As the ministry of health labors on the seriousness of NCD’s, to tackle it does not only involve the reform in health. The neighborhood and built environment plays a crucial role in enabling the practice of a healthy lifestyle. We tell people to exercise yet there are no safe paths within the vicinity of the community, no proper bike lanes, poor roadworks that support pedestrian and bicycle use, and poor facilities for hiking trails and nature reserves.
Stunting (low height for age) of our children below 5 years old has increased from 13.4% in 2015 to 21.8% in 2019. Short term effects of malnutrition includes impaired brain development, lower IQ and a weakened immune system with recurrent infections, whilst in the long term it leads to shorter adults, greater risk of NCDs, lost productivity and increased healthcare costs and premature deaths.
There are multiple compounding factors which needs to be addressed holistically which goes beyond the MOH reform agenda. This includes addressing the low-income status of families, alleviating poverty, better housing, better social security safety net, better health education, ensure food security which are all social determinants of health. The reformed healthcare system should invest better in preventative healthcare services (68% of total health expenditure spent on curative care services in 2018) which would ensure good antenatal care, exclusive breastfeeding in the first 6 months of life, optimum complementary feeding in the first 2 years of life and optimize family based diet for the 2-5 year olds.
The collaboration and synergy of multiple ministries and agencies are essential to ensure success of nurturing the good health of our youngest and most vulnerable within the context of the HiAP government philosophy. [10]
There are 3 major areas in the healthcare ecosystem that need to be reformed, namely, transformation of the public health sector, regulatory reforms of the private health sector enabled by sustainable healthcare financing as illustrated the following diagram XI
Diagram XI:

This new paradigm in healthcare is captured in the maxim “Technology-native, person-centered integrated care, based on value and choice, supported within a health empowering ecosystem”
And as the dictum goes, health is wealth. Good health leads to the people’s well being, enhances their productivity and better contributes to the wellbeing and prosperity of the nation.
References:
- https://www.nst.com.my/news/nation/2022/04/785239/kj-white-paper-healthcare-reform-be-tabled-parliament-soon
- https://krinstitute.org/assets/contentMS/img/template/editor/KRI%20-%20Presentation%20Slides.pdf
- https://iptk.moh.gov.my/images/technical_report/2020/4_Infographic_Booklet_NHMS_2019_-_English.pdf
- https://www.theedgemarkets.com/article/audit-finds-malaysian-hospitals-understaffed-underfunded-and-overcrowded
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)30818-8/fulltext
- https://www.malaysiakini.com/columns/616966
- https://www.who.int/publications/i/item/9789241500852
- https://journals.sagepub.com/doi/full/10.1177/0169796X211041154
- https://academic.oup.com/heapro/article/29/suppl_1/i19/646334?login=false
- https://codeblue.galencentre.org/2022/05/23/children-food-and-nutrition-why-are-our-children-malnourished-prof-dr-muhammad-yazid-dr-musa-mohd-nordin/

