
The suggestion by the deputy minister of health for the MOH to pause vaccine shots at night during Ramadan must not be seen in isolation. It must be discussed within he context of the burgeoning COVID-19 cases and the need to achieve population immunity.
Malaysia has the highest cumulative cases per million in the ASEAN region at 11 thousand cases per million population. Even corrected for the COVID-19 testing differences, we are more than Singapore (10K), Philippines (8K), and Indonesia (6k).
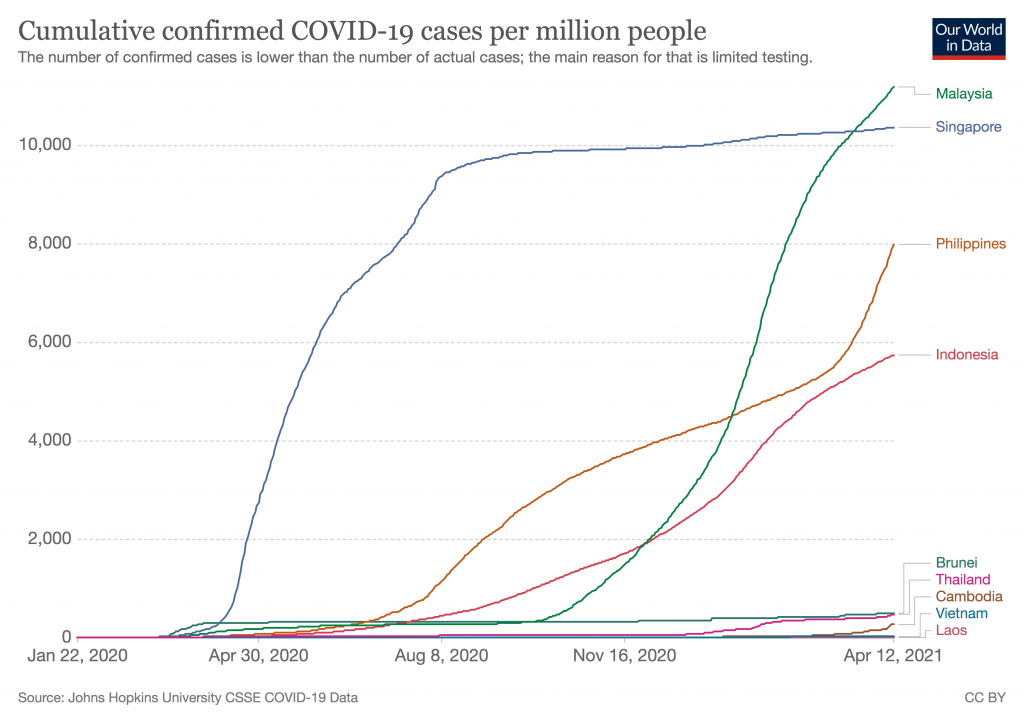
The MOH is reporting 1 – 2 thousand cases per day, with 188 cases in the ICU and 84 cases on respiratory support.
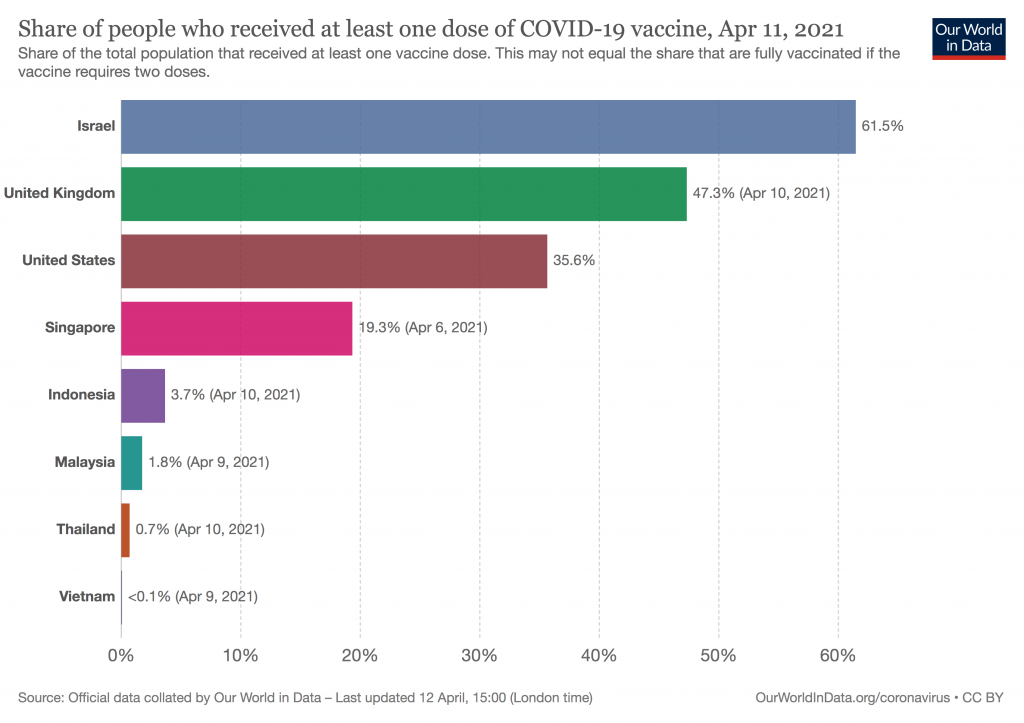
Our vaccination uptake for one dose is only 1.8%, whilst Indonesia is ahead at 4% and Singapore, 10 times more at 19%.
The MOH is predicting a fourth wave and when it arrives I think it will be even more devastating with the spread of COVID-19 variants which are more resistant to the available vaccines, namely the B117 (UK) and B1351 (South Africa) strains.
And Europe, South America, North America, and India is weathering through this punishing new variant COVID-19 wave.
With these grim statistics, it goes without saying that we must warp speed the rollout and scale up the coverage of the COVID-19 vaccines
The coronavirus is blind as to whether it is Ramadan or Hari Raya People get infected, admitted into hospitals, and succumb to death regardless of whether it is Ramadan or Syawal. Thus the vaccine rollout should proceed as planned
The concern that people won’t show up for the vaccines because it might clash with terawih prayers needs to be carefully addressed with caution and sensitivity.
It must be however noted that the terawih prayers are not mandatory prayers. They are nonetheless a strong practice, tradition and sunnah of the Prophet and his companions (peace be upon them)
There is a perplexing contradiction of sorts in our Malaysian Muslim religiosity. They throng to the mosques during the month of Ramadan to perform the optional terawih (sunnat muakkad) but the mosques are relatively empty during the mandatory 5 day prayers, including the night maghrib and isya’ prayers
Studying from the perspective of the maqasid shari’ah (the higher objectives of the Islamic jurisprudence), universal COVID-19 within the ambience of the raging pandemic, is to fulfill the maslahah ammah (benefits of the larger community). And it is a fiqhi (jurisprudential) ruling that that general public interest shall take priority and precedence over maslahah fardhi (individual benefits).
Therefore, a smart compromise must be crafted to ensure that the vaccine rollout is not negatively impacted by the religious practices during the blessed month.
In this context, the Muslim Malay leaders, notably the Muslim religious scholars have to be exemplary. Instead of politicizing the issue along religious sentiments, the Minister of religion and the Muftis should rally for the immunisation campaign during the month of Ramadan. Instead of making trips abroad for meetings or to perform the umrah, they should instead be addressing the pressing needs of the community. Some of the Malay Muslims may not even want be vaccinated during the day let alone the nights. These are the demands of Fiqh Awlawiyat, the jurisprudence of priorities, to ensure that the national vaccine roll out is preserved within the realm of reducing the burden of COVID-19 disease in the community
What a better show of confidence in the national vaccine campaign than to see the Muftis and the asatizah (Muslim religious scholars) taking the lead in getting their COVID-19 vaccines during phase 2 in the month of Ramadan.
The JKJAV and some vaccine authorities has screamed all along about ensuring the equitability of the vaccine roll out. Now the test is before us. Should our co-religionists, non-Muslims, be similarly excluded from the shots during Ramadan nights just because their Muslim colleagues are busy engaged in Terawih prayers?
If the Muslims are allowed to opt out during the nights of Ramadan, the non-Muslim should not be penalized but allowed to continue with their shots.
Whilst on the topic of equitability, why should the 30 thousand or so of young (less than 50 years old) to be pilgrims, jump the queue and take precedence over the higher risk senior citizens and those with co-morbidities? The JKJAV, the Ministers at MOSTI and the MOH needs to address this gross infringement of equity vis a vis COVID-19 vaccines distribution. If they can fork out RM20 thousand or more for the Hajj, they should be made to pay for their vaccines in the private health care and the Minsters have no legitimacy nor credibility to short circuit the long COVID-19 vaccine queue for them.
The strongest religious opinion and it is a very strong consensus among Muslim scholars that injections, like the COVID-19 shots does not nullify the fast.
Muslim adults are advised to prepare for the upcoming jab during Ramadan, by ensuring that they are well hydrated and consume a proper meal during the sahur (waking up before dawn for a meal which is another strong tradition of the Prophet).
The elders who are beyond 65 years old, should be in good health and those with co-morbidities should see their respective family physicians to ensure that their conditions are well controlled. Unless this is attained, we should delay some of those with pre-existing disorders to after Ramadan
In the exceptional circumstances, where they develop adverse effects following immunisations (AEFI) which are not tolerable, they can break their fast.
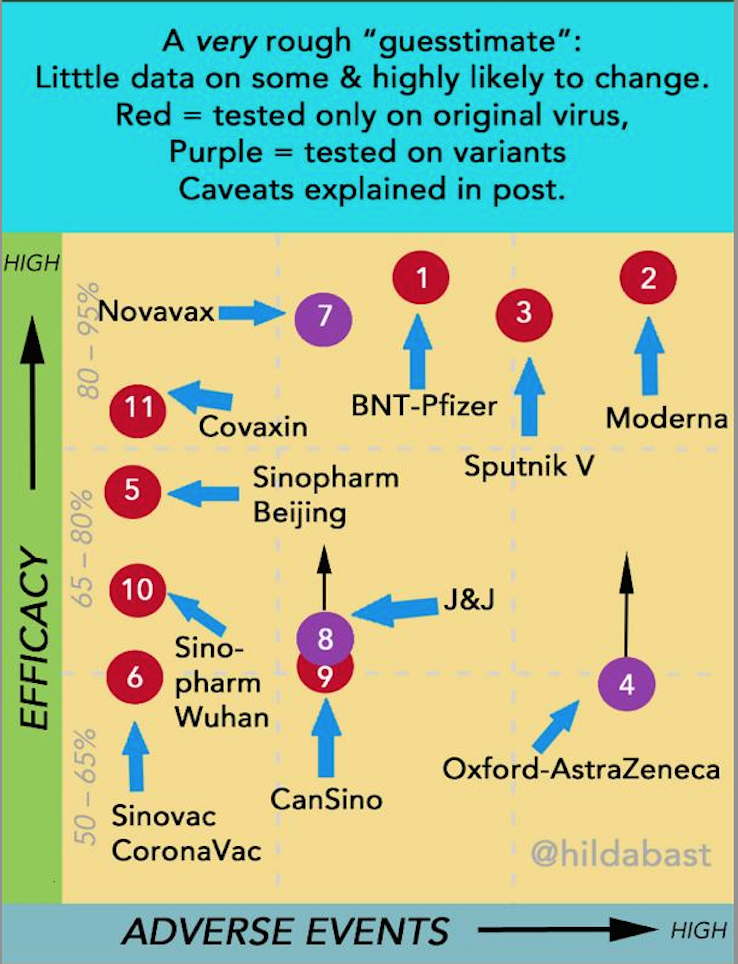
It needs mentioning that the Sinovac vaccines, though less efficacious (Vaccine Efficacy of 50-83% but effective against severe COVID-19 and deaths) have less AEFI when compared with the Pfizer vaccines.
If the public can flock to the Bazar Ramadan, I think there is no plausible excuse for them to refuse vaccines. The over-eating often seen at the break of fasting and the smoke particles from the ayam percik at these Bazars is probably more detrimental than the AEFIs of the COVID-19 shots.
There is no precedent of adult vaccination in the MOH National Immunisation Program, except for tetanus vaccination in pregnant mothers.
Virtually all adult vaccinations are done by private GPs, family doctors and in private hospitals e.g. influenza, pneumococcal, meningococcal, shingles and varicella vaccinations.
I have since the initiation of the vaccine rollout on 24 Feb 2021, advocated for the early engagement of the private health care sector rather than later in September 2021 as mentioned by the JKJAV. This is a pandemic, a national emergency (the PN government has even declared it a Darurat by Emergency Ordinance). An Emergency situation demands emergency solutions i.e. mass vaccine rollouts at warp speed not turtle speed like presently.
My first suggestion to the NPRA is to issue similar Emergency Use Authorization (EUA) licensures to the Moderna, Sputnik V, Janssen and Novavax vaccines which have been published in peer reviewed scientific journals and has been used in well over 30 countries (1,2,3).
This will allow Malaysia to have access to a wider portfolio of vaccines, utilizing different platforms of modus operandi.
When the Indian public healthcare facilities rolled out the vaccines, they managed 300,000 doses per day. When the private facilities were involved they managed to increase it by 7 times, i.e. 2 million doses per day.
The second suggestion is to ramp-up the administration of the vaccines, as shown by the MOH in Israel and UAE from Day 1 of its rollout programme. We do not compare ourselves with Singapore, Australia or New Zealand, who can all take their own time since their COVID-19 incidence is virtually zero. Singapore had only 1 case of indigenous community spread for the 2-week period 12-25 Mar 2021 (4)
Thirdly, this is not helped by a MySejahtera app which is not at all user-friendly. I had to get my tech-savvy daughter to do a third registration for me. Imagine the difficulties that others in the rural communities might experience. It is thus not surprising that the registration numbers of the citizens are well below expectation. Others initiatives like Selangor’s ImuniSel outreach program to increase the registration of Selangorians needs to be undertaken.
It is even worse for those in the East Coast states and Sabah. Other contributory factors needs to be considered, including the backdrop of low childhood immunisation uptake in these states. The 2019 uptake of the 1st dose MMR was less than 85% in both Kelantan and Terengganu, compared to the national average of 95%. The overbearing influence of extreme religious sentiments must be addressed by the authorities, despite the national fatwa by the Minister of Religion.
Next, the JKJAV should allow the APHM, states and other stakeholders to begin to procure vaccines which are not within the JKJAV portfolio, for example the Moderna vaccines. Unlike suggestions by a few specialists, the APHM is not pinching the MOH vaccine stockpile. It is over and above that.
They would be able to address the immediate and critical needs of the following cohorts, namely;
- expatriates
- young businessmen who need to travel
- students undertaking overseas studies
- those who would like a choice of the type of vaccines
- T20 citizens who do not mind paying
- migrant workers and refugees which some state government would like to prioritize to protect their industries and high risk groups
- those going for hajj should not be allowed to jump queue, instead get their shots in the private sector etc
Not only will this ensure warp speed, preserve equity, it would enhance coverage and allow for faster attainment of the 70-80% herd immunity. And to facilitate this national vaccine agenda, the ceiling price of the vaccines must be set to protect against criminal profiteering by connected cronies and the private healthcare facilities.
References:
- https://www.who.int/news/item/12-03-2021-who-adds-janssen-vaccine-to-list-of-safe-and-effective-emergency-tools-against-covid
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00234-8/fulltext
- https://www.nejm.org/doi/full/10.1056/NEJMoa2035389
- https://www.moh.gov.sg/docs/librariesprovider5/local-situation-report/situation-report—20-mar-2021.pdf
Dr Musa Mohd Nordin
14 April 2021

